
CT in AcuteAbdominal Pain
Mindy M. Horrow, MD, FACR
Director of Body Imaging
Albert Einstein Medical Center
All photos retain the copyrights of their original owners
© Mindy Horrow, MD
•Technique
•Gastrointestinal Tract
•Pancreas
•Biliary System
•Spleen
•Genitourinary Tract
•Vascular System
CT Protocol
•Intravenous contrast
•Oral contrast
•Timing, acquisitions
•Collimation
*Clear communication betweenradiologist, patient and referringclinician is essential to narrowdifferential diagnosis and tailor CT exam
Introduction
•Acute abdomen: Severe abdominalpain developing rapidly
•Fast, accurate diagnosis essential todecrease morbidity and mortality
•CT has accuracy of 95% in thesepatients
Taorel et al: Gastrointest Radiol 1992; 17:287
Siewert et al: AJR 1997; 168:173
Mindelzun et al: Radiol 1997; 205:43
Urban et al: RadioGraphics 2000; 20:725

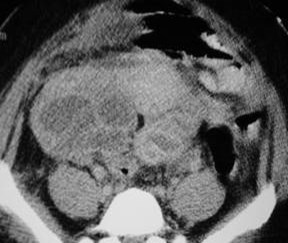
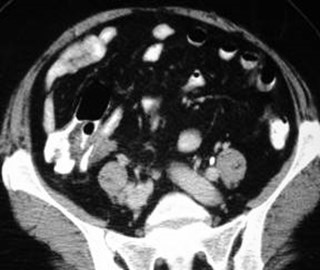
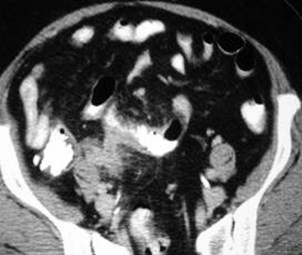
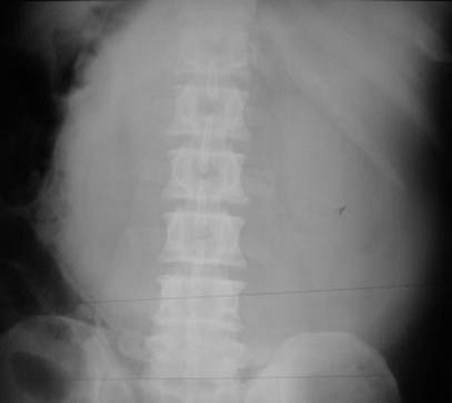
Small BowelObstruction dueto femoral hernia
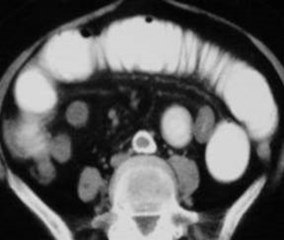
Small Bowel Obstruction
•For high grade obstruction, sensitivity 90-96%, specificity 96%
•Low grade obstruction - sensitivity 50% andmay require barium study
•Causes:
Adhesions (64-79%)
Hernia (15-25%)
Tumor (10-15%)
Megibow et al: Radiology 1991; 180:313
Maglinte et al: Radiology 1993; 188:61
CT Findings ofSmall Bowel Obstruction
•Decompressed colon
•Transition from dilated tonondilated small bowel
•When no obstructing mass orhernia, most likely cause isan adhesion


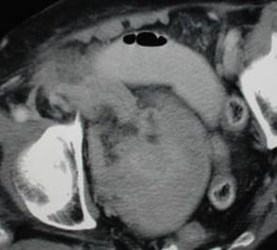
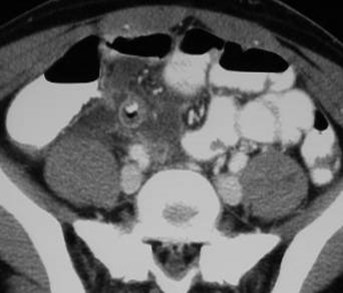
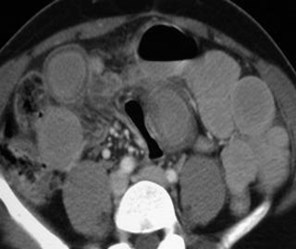
Closed loop small bowel obstruction
with early signs of ischemia
Simple vs. Strangulated SBO
•Caused by obstruction of proximalbowel 2° closed loop obstruction withvenous congestion of involved loop
•Venous congestion vesselengorgement bowel hemorrhage fluid transudates into peritoneum
Simple vs. Strangulated SBO
•Findings:
Poor bowel wall enhancement
Twisting of mesenteric vasculature (beaksign)
Peculiar C or U shaped bowel configuration
Mesenteric edema
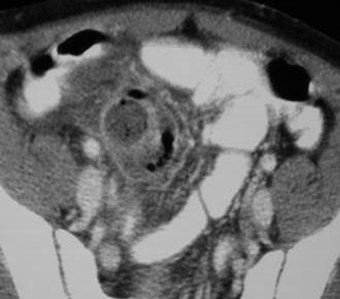
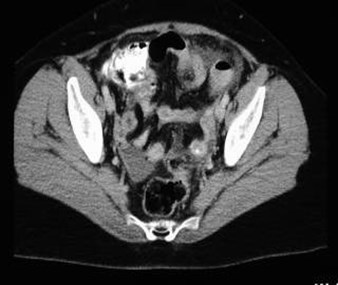
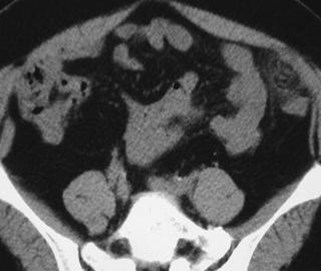
Appendicitis
Appendicitis
•CT Findings:
Dilated appendix (> 6 mm)without filling by oral contrast
Periappendiceal inflammation
Increased enhancement of wall
Appendicolith
•Accuracy 94-98%
Ruptured
Appendicitis
Rupturing appendicitis

Perforated Appendicitis
•Extra-luminal air
•Extra-luminal appendicolith
•Abscess
•Defect in enhancing wall
•Phlegmon
* More common in the elderly
Horrow, White et al: Radiology (in press)
Sigmoid diverticulitis
With rectal contrast
Cecal diverticulitis with
perforation

Diverticulitis
•93% sensitive, near 100% specific
•Much more sensitive than barium enemabecause CT can visualize the pericolonicprocess
•CT findings: inflammation adjacent tocolon with diverticula, often wallthickening. May also see phlegmon,extra-luminal air or abscess
Cho et al: Radiology 1990; 176:111
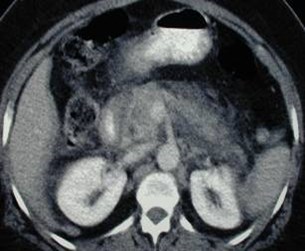


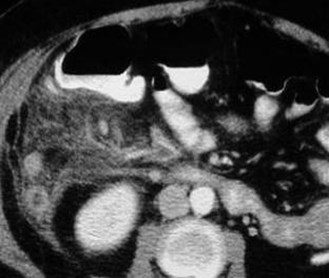
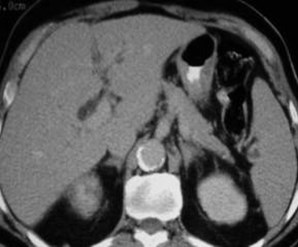
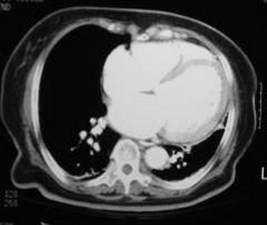
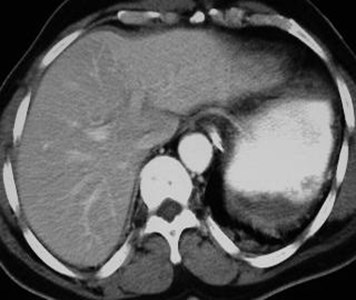
AcutePancreatitis



Hemorrhagic
Pancreatitis



Acute Pancreatitis
with splenic arterypseudoaneurysm
Splenic artery
PSA
PSA
Acute Pancreatitis
•CT findings correlate well with severity ofdisease, predicts clinical outcome
•Findings include: focal/diffuse enlargement,peripancreatic inflammation, areas ofdecreased attenuation necrosis, phlegmon,peripancreatic collections, hemorrhage,abscess
Acute Pancreatitis
•Vascular complications: splenic veinthrombosis or splenic arterypseudoaneurysm
•Technique crucial: IV contrast, timing
Balthazar: Radiology 2002; 223:603

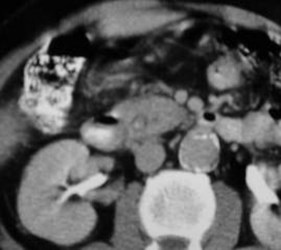
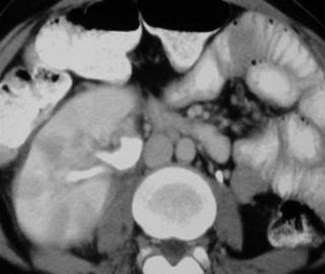
Choledocholithiasis
w biliary dilatation
S/p cholecystectomy


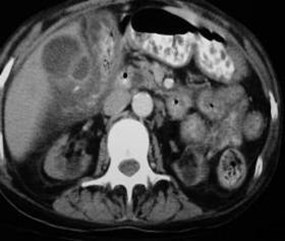
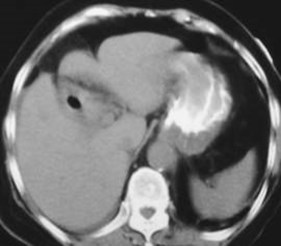
Acute Cholecystitis
with
Ruptured Gallbladder

Gallstone Ileus
Biliary System
•Acute cholecystitis: inflammation, wallthickening/enhancement, calculi,distention.
However, CT can be relatively unremarkable
•Choledocholithiasis: high attenuationnidus in duct, dilated ducts

Spleen
•Infarction: wedge shapedareas of decreasedattenuation extending tosurface, if diffusely hypo-attenuating may be globalinfarction
Genitourinary Tract
•Acute Pyelonephritis
•Renal Infarction
•Ureteral Calculi
•Pelvic Inflammatory Disease

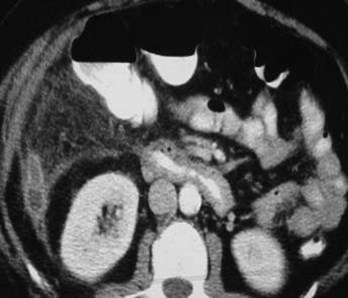
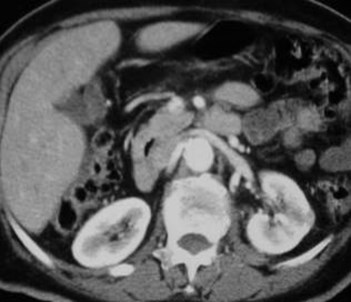
Acute Pyelonephritis
Acute Pyelonephritis
•Protocol: IV contrast, 1-2 acquisitions
•CT findings: striated/wedge shapedareas of hypoperfusion, renalenlargement, perinephric inflammation.Delayed views may demonstrate areasof increased attenuation

Patient with atrial fibrillation
Left atrial thrombus
Renal infarct
Renal Infarction
•Due to: embolism, aortic dissection,trauma, thrombosis, trauma
•Protocol: IV contrast, early acquisition
•CT findings: focal parenchymaldefect(s) involving cortex and medullabut not capsule, may be global


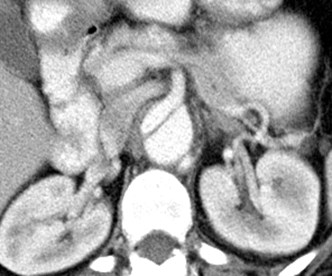
Patient with right flank pain
Mild right renal enlargement
& hydronephrosis
Mild hydroureter
Right ureterovesical junction calculus
supine
prone
Ureteral Calculi
•Technique: no oral or IV contrast, narrowcontinuous slices
•Sensitivity 97%, specificity 96%
•CT findings:
1° - hydronephrosis, hydroureter, obstructingcalculus
2° - perinephric stranding, renal enlargement
•Other diagnoses
Smith et al: AJR 1996; 166:97

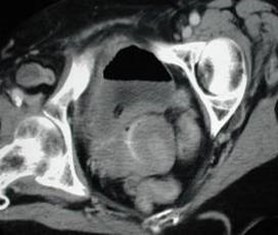
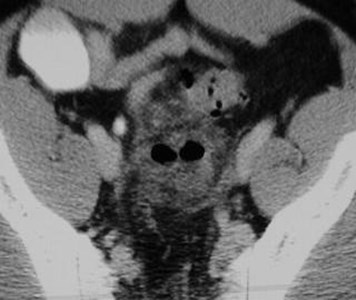
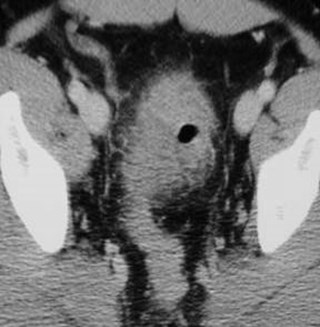
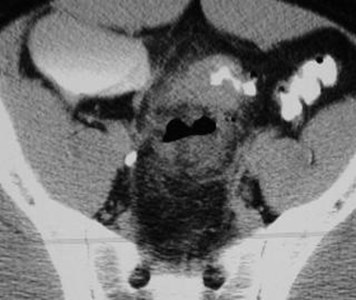
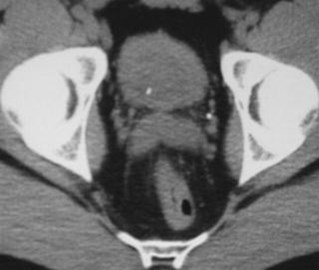
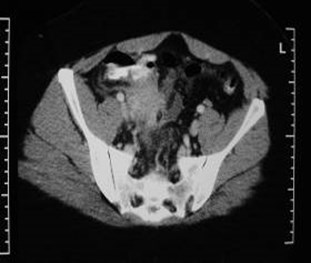
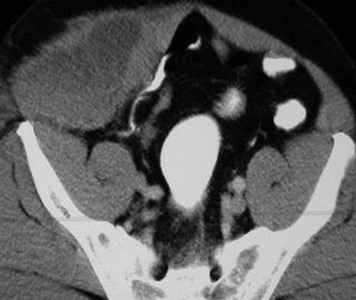
Pelvic inflammatory disease
with left pyosalpinx and
cul-de-sac collections
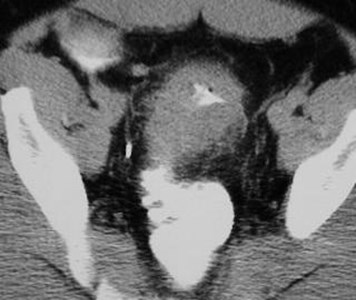
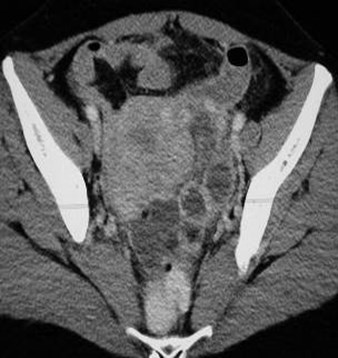
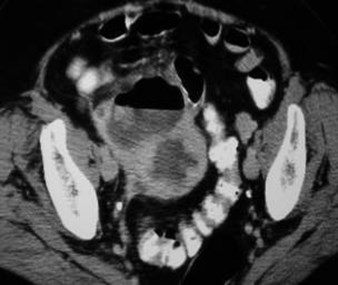
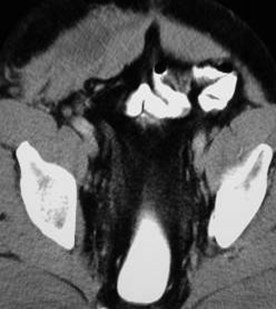
Bilateral pyosalpinges


Bilateral TOAs
with peritonitis
and hydronephrosis
Pelvic Inflammatory Disease
•Ultrasound is primary modality
•Technique - oral / IV contrast
•CT findings: pelvic inflammation,unilateral/bilateral adnexalmasses, hydrosalpinx, ascites.Findings overlap with otherdiagnoses.
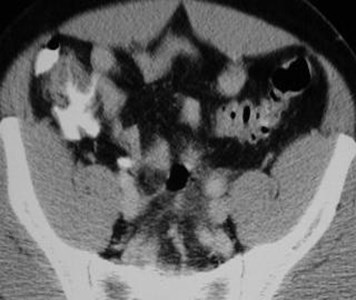
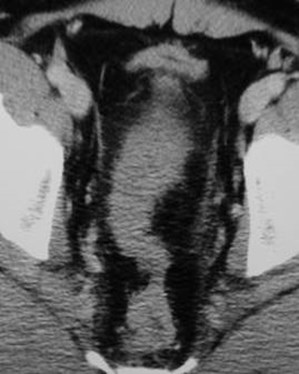
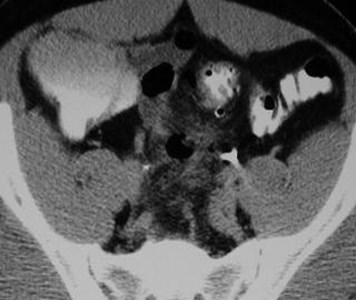
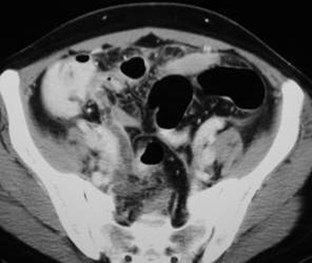
PID vs. Appendicitis
•Missed appendicitis
•Missed perforated appendicitis
•Appendiceal abscess vs. TOA
•Ruptured appendicitis causing TOA

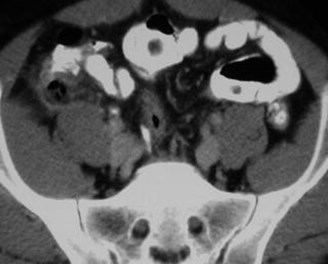
Missed appendicitis- enlarged appendix
appears similar to small bowel loops


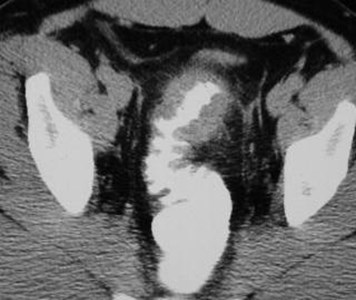
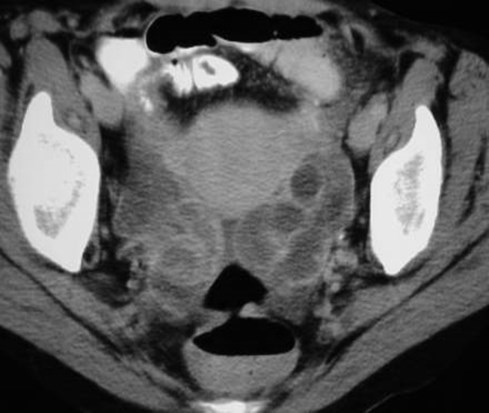
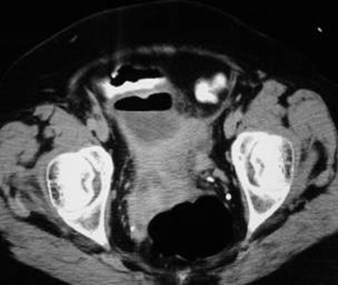
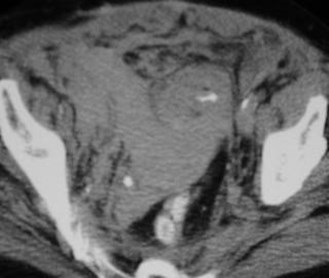
Initially interpreted as
bilateral pyosalpinges
with free fluid
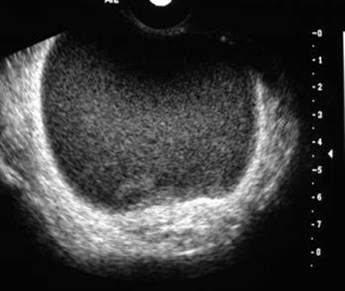
One week later after appropriate outpatient
antibiotics, symptoms persisted
Pelvic US showed normal ovaries and pus in cul-de-sac= ruptured appendicitis
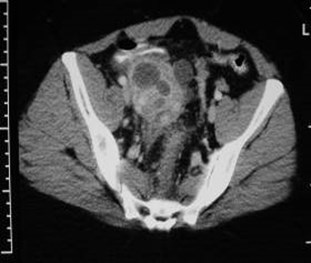

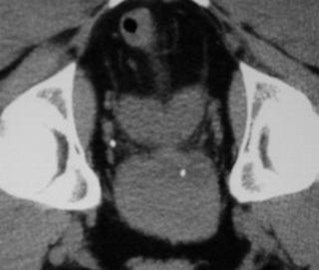
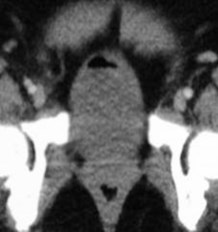
TOA or
Appendicealabscess?
RLQ pain with fever for several days
right TOA and pyometra
68 year old with abnormal appendix

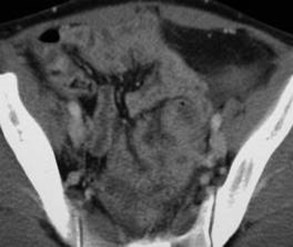
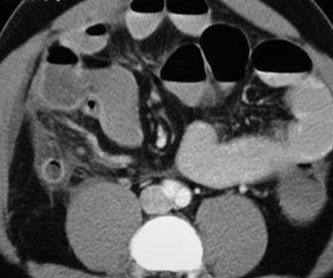
Small bowelobstructionwith earlyischemia



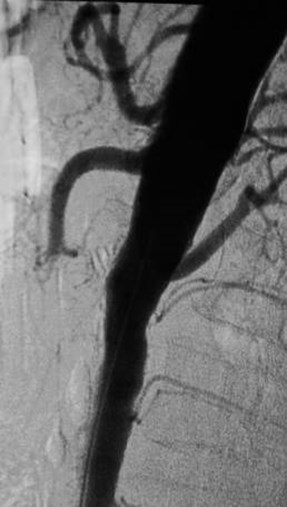
Patient with atrial
fibrillation and acute
abdominal pain
SMA embolism with
complete thrombosis
and subsequent
bowel infarction
Bowel Ischemia
•Causes: vascular occlusion/thrombosis - arterial/venous,hypoperfusion. May also resultfrom vascular compromise 2° bowelobstruction, hernia,intussusception
•Sensitivity ~80%, findings ofischemia may be nonspecific
Bowel Ischemia
•CT findings: non-patent vessels,bowel wall thickening with lowattenuation edema; air in bowel wall,mesentery or portal veins; thoughpneumatosis not specific forischemia.
Frager et al: AJR 1996; 166:67
Balthazar et al: Radiology 1997; 205:519


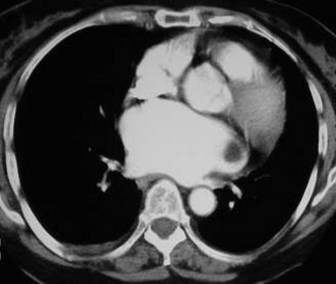
Ruptured aortic aneurysm
Vascular System
•Aortic Aneurysm Rupture
•Aortic Dissection
•Hemorrhage
Aortic Aneurysm Rupture
•Technique: CT angiography withmultiplanar 20/30 reconstructions;rapid IV bolus with narrow collimation,no oral contrast
Aortic Aneurysm Rupture
CT findings: retroperitoneal hematoma,contrast extravasation, if impendingrupture may see > 1 cm increase inaneurysm in 6 mos, draped aorta sign,high attenuation crescent, break-incalcified rim

Aortic Dissection
Courtesy of UNC Radiology Teaching File
Aortic Dissection
•Defined as hematoma in wall,typically with tear in intima
•CT is screening modality ofchoice with nearly 100%sensitivity, requires CTangiography technique
Aortic Dissection
•CT findings: contrast in 2 channelswith intervening intimal flap. If onelumen is thrombosed may bedifficult to differentiate from muralthrombus
Sebastian et al: RadioGraphics 1999; 19:45
Aortic Dissection
•Associated findings includecompressed true lumen, differentialrenal flow, ischemia/infarction inaortic branches
Sebastian et al: RadioGraphics 1999; 19:45


Acute hematoma in
Anterior abdominal wall muscles

Hemorrhage and ATN after catheterization
Vicarious gallbladder
excretion & delayed
nephrograms
Extra & retroperitoneal
hemorrhage
Hemorrhage
•Technique: initial unenhanced CT,then angiographic technique asneeded to detect site of acutebleeding
•Locations: bowel (coagulopathies),musculoskeletal (spontaneous),retroperitoneumLane et al: AJR 1998; 171:679
Potpourri


Emphysematous
pyelonephritis &
cystitis

Epiploic Appendigitis
Acute abdominal pain with vomiting



Gastricvolvulus



Large bowelobstruction
Secondary to intussusception
with a malignant polyp & livermetastases
The End